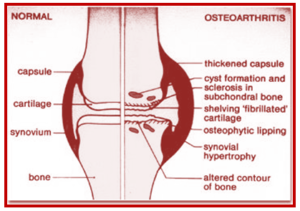
If you are in your late 40 years or older, overweight, Young sportsman with any knee injury, or had knee operation in the past, or your parents or siblings had Osteoarthritis or you’re experiencing the below symptoms, it is time you look for a treatment before the condition named as Osteoarthritis makes you stall.
- Vigorous pain, particularly when you move the knee or at the end of the day.
- Stiffness in the joints, especially after long rest which might ease out as you get moving or after few minutes.
- A crunching, grinding sensation as you move your joint.
- Hard and soft swelling of the joints.
- Knee Joints is becoming less stable and Muscle weakness around the joint.
- You are not able to move your knees as freely as before.
- Your knees becoming bent and bowed
- Change in Pain severity during damp weather and low pressure with stiffness worsening.
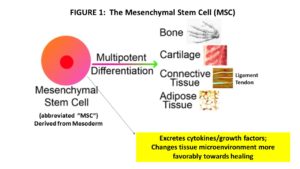
An inflammatory milieu breaks down the cartilage matrix and induces chondrocyte apoptosis, resulting in cartilage destruction in patients with cartilage degenerative diseases, such as rheumatoid arthritis or osteoarthritis. Because of the limited regenerative ability of chondrocytes, defects in cartilage are irreversible and difficult to repair. Mesenchymal stem cells (MSCs) are expected to be a new tool for cartilage repair because they are present in the cartilage and are able to differentiate into multiple lineages of cells, including chondrocytes. Although clinical trials using MSCs for patients with cartilage defects have already begun, its efficacy and repair mechanisms remain unknown.

Figure 1. Strategies for efficient cartilage repair therapy by intra-articular injection of mesenchymal stem cells (MSCs). The inflammatory environment is present in the joints affected by rheumatoid arthritis (RA) or osteoarthritis (OA). Chondrogenic differentiation of intra-articular injected MSCs is inefficient under inflammatory conditions. Therefore, pre procedural treatment with anti-inflammatory drugs and/or chondrogenic agents should be important for efficient cartilage repair therapy.
The inflammatory milieu is known to cause cartilage destruction by causing disturbances in the anabolic/catabolic balance of the cartilage matrix. The inflammatory milieu has also been understood to exert a suppressive action during the process of differentiation from progenitor MSCs to chondrocytes. Therefore, sufficient suppression of articular inflammation prior to a procedure may be important for efficient regeneration of the cartilage in regenerative therapies using MSCs. While continuous studies to develop more efficient techniques for chondrogenic differentiation using MSC-based cell therapies are important, it is necessary to establish a protocol for the improvement and maintenance of the intra-articular environment, where MSCs are transferred, to be suitable for cartilage regeneration.
In several clinical trials(1), MSCs injected into the joints by the least-invasive intra-articular method, and were expected to differentiate into chondrocytes locally in the joint. Whether or not the intra-articular environment of the joints was suitable for chondrogenic differentiation of MSCs is a major concern. As mentioned , cartilage regenerative therapy is likely to be indicated when the affected joints in patients with OA and RA present with inflammatory reactions. However, the inflammatory milieu, including proinflammatory cytokines, strongly inhibits MSC differentiation into chondrocytes. On the other hand, it has been demonstrated that the influence of inflammation (pro inflammatory cytokines) on MSC is differentiation into osteoblasts, resulting in the formation of calcifications. These findings may indicate the risk of developing osteophytes and ectopic calcifications when MSCs are injected into the joint in an inflammatory milieu. Therefore, sufficient suppression of articular inflammation prior to any procedure is important for efficient cartilage regeneration while using MSCs in cartilage regenerative therapy. This can be achieved by a combination of an existing anti-inflammatory agent or a biologic targeting proinflammatory cytokine and a chondro-enhancing agent (Figure 1).
1. Acquiring Chondrocyte Phenotype from Human Mesenchymal Stem Cells under Inflammatory Conditions
Masahiro Kondo, Kunihiro Yamaoka and Yoshiya Tanaka
Int J Mol Sci. 2014 Nov; 15(11): 21270–21285.